Document Type : Original Article
Authors
1 Research Scholar, KIIT School of Management, KIIT Deemed to be University, Bhubaneswar, India
2 Professor, School of Management, KIIT Deemed to be University, Bhubaneswar, India
3 Senior Professor, School of Management, KIIT Deemed to be University, Bhubaneswar, India
Abstract
Humanitarian emergencies including disasters associated with natural hazards, conflict, complex emergencies, and famines can pose significant risks to public health, especially when they lead to population displacement into inadequate conditions. To reduce the risk of communicable disease (CDs) outbreaks in such situations it is necessary to know the key risk factors. In recent times, communicable diseases are the number one cause of disability and death around the globe. The communicable disease can be controlled by creating awareness of the symptoms and types and possible risk factors. Given that the relevance, especially for the paramedic staff of various hospitals was considered. As we know due to the internal dynamics of the nature of work these paramedic staffs have to pass a lot of stress and untimely eating habits along with other unwanted habits especially male paramedics like cigarettes, and alcohol, etc. The purpose of the study was to examine awareness level on Communicable Diseases (CDs) among paramedics in the private healthcare sector in India. The analysis for CDs done for decoding the awareness level in three parameters such as symptoms of CDs, types of CDs, and risk factors of CDs, by taking three important pillars of paramedics: nursing practitioners, physician’s assistants, and emergency medical technicians. In the beginning 34 variables were identified, however, after the pilot study and core group discussions, the number of attributes for the CDs restricted to 24 only. The results show that in the case of CDs, there is need for improvement of awareness among the respondents for symptoms and mixed results for other factors.
Graphical Abstract
 Among Paramedics in Pr ... ', 'data/jmcs/coversheet/711679137570.jpg'))
Keywords
Introduction
Providing clinical services under the supervision of a physician is what paramedical personnel, also called paramedics. It is usually associated with nurses, therapists, technicians, and other ancillary personnel involved in health care. However, it is frequently used to refer to highly skilled individuals who are directly responsible for patient care alongside physicians. A nurse practitioner, physician's assistant, or emergency medical technician falls into this category. They relieve physicians of conducting routine health assessments and taking medical histories by performing routine diagnostic procedures, such as taking blood samples. In addition, they perform therapeutic procedures, such as administering injections or suturing wounds. It is less comprehensive than the education required of physicians and prepares individuals to fill speculative healthcare-care roles.
Communicable diseases are one of the primary concerns in humanitarian emergencies and disasters [1]. Humanitarian emergencies include disasters associated with natural hazards such as earthquakes, floods, and tsunamis, as well as man-made disasters such as famine, conflict, and complex emergencies. These emergencies usually require a large-scale international response and affect large proportions of a community, country, or region. The importance and overall risk of communicable diseases and communicable disease outbreaks differs between different disaster types. It is particularly low in geo-disasters such as earthquakes or volcanic eruptions [2], higher for flooding [3], and much worse again in refugee crises [4], or complex humanitarian emergencies [5]. While the problem of a potentially increased risk of communicable diseases in humanitarian emergencies is well documented, information on specific risk. Factors and the levels at which these risk factors become critical is lacking. Yet, the identification of risk factors and their interaction is crucial for risk management. Knowing the overall risk profiles can help identify those sites where proactive interventions may reduce the impact of communicable diseases. Key risk factors for communicable diseases identified in the academic literature can be broadly grouped into categories such as Water, Sanitation and Hygiene (WASH), health and public health system, environment, humanitarian response, infrastructure, insecurity, living conditions, nutrition, mass population displacement, and economy [6]. Within those broader categories, individual risk factors are defined more specifically, although the categories themselves serve as general risk factors as well [7]. While similar groups of risk factors have been identified as significant for all emergency types, their weights can differ depending on the individual setting as does the overall risk of a communicable disease outbreak. The risk of communicable disease outbreak is almost negligible in geo-disasters that do not trigger a secondary disaster such as a displacement crisis. For each site, it is also important to know which risk factors are of the most pressing concern to allocate resources correctly and prioritize interventions [8].
Need for the study
As we know paramedics are the most vulnerable group in health care services and they are the front-line workers for the health care delivery system. The same being tried and tested during recent pandemic. During interaction with these paramedics, and review of various previous studies, it was also observed that very limited study being conducted on communicable diseases (CDs) in the study areas specially related to symptoms, types of communicable diseases, and risk factors related to the same.
Research questions
What are the various factors that lead to Communicable Diseases (CDs)?
What are the various diseases related to CDs?
What is the awareness level among the paramedic staff in the private healthcare sector on CDs?
Objectives of the study
- To study various factors that lead to communicable diseases.
- To understand the awareness level of communicable diseases among paramedics in the private health care sector.
- To contribute to the existing literature.
Scope of the study
The present study is limited to the health care workers of private health care providers in the eastern region of India. They include nurses, therapists, technicians, and other ancillary personnel involved in medical care but are frequently applied specifically to highly trained persons who share direct responsibility for patient care with physicians.
Methodology of the study
Both primary and secondary data were used in this study. Research gaps were identified using the secondary data. Sampling was conducted randomly. A literature review and seven core group discussions with seven members each were conducted to identify the communicable diseases (CDs) 34 attributes initially considered. However, after the core group discussions and pilot study, 24 final variables were retained. 54 respondents were considered for the pilot study purpose in the study area. This study used a Likert-type five-point scale method to compute data along with analysis of variance, with scores of 4 for Completely Aware (CA), three for Aware (A), two for Neutral (N), one for Not Aware (NA), and zero for Completely Not Aware (CNA). Data under 3 parameters are computed using perception weights for the communicable diseases (CDs).
Sample size determination
A sample size of 1:4 to 1:10 was calculated in the present study (Rummel, 1970). The present study determined that the minimum sample size should be 4 times the number of items, while the maximum sample size should be 10 times the number of items. In the present case, 24 attributes for the communicable diseases (CDs). In the present case, one should expect the sample size of the minimum sample size 96 and maximum should be 240, Taking 217 observations within the minimum and maximum sample sizes above after removing the common outlier result in a sample size of 217. Our study is adequately sampled based on Rummel (1970) and Schwab (1980).

With reference to Table 1, in overall 217 responses collected as against questionnaire distributed 330. It includes 125 from Bhubaneswar, 28 from Cuttack, 27 from Berhampur, 24 from Rourkela and remaining 15 from Dhenkanal region.
Figure 1 presents various communicable diseases such as virus, bacteria, protest, fungi along with others.
With reference to Table 2, the scores were computed by considering the following equation:
The maximum possible score = the number of responses X Number of variables X maximum possible weight, The least possible score = the number of responses X number of variables X least possible weight.
Figure 2 explains the percentage of total weight to the maximum possible weight.
Figure 3 represents the percentage of total weight to total possible weight for the awareness of types of communicable diseases.
Figure 4, represents percentage of awareness to maximum possible weight.



Results and Discussion
According to Table 3, responding to the awareness of symptoms of Communicable Diseases (CDs), the percentage of total weight to maximum possible weight were 52.65, 63.71, 54.56, 65, 61.46, and 58.90 for NPM, NPF, PAM, PAF, EMTM, and EMTF, respectively. Its average weight was 59.38%. This shows that the NPM, PAM, and EMTF weight are the below average. It also clear that majority are aware of symptoms like fever, cough, difficulty in breathing, and vomiting. However, very less awareness on fatigue, body aches, nausea, diarrhea, rash, and painful stores in skins.
According to Table 4, responding to the variables of awareness on types of Communicable Diseases (CDs), the percentage of total weight to maximum possible weight were 72.55, 70.24, 86.76, 87.61, 76.74, and 86.69 for NPM, NPF, PAM, PAF, EMTM, and EMTF, respectively. The average weight for this was 80.10%. This shows that PAM, PAF, and EMTF having more than average weight and other groups are less than the average weight. This indicates the respondents of the study area highly aware of COVID, bacterial infections, fungal infections, and viral infections. However, there is less awareness level for the parasitic infections and prion infections.
Based on Table 5, joining to the questions of awareness on risk factors of Communicable Diseases (CDs), the percentage of total weight to maximum possible weight were 73.93, 77.43, 84.71,88.42, 65.80, and 64.61 for EMTF, EMTM, PAF, PAM, NPF, and NPM, respectively. The average weight is 75.82 percentage.

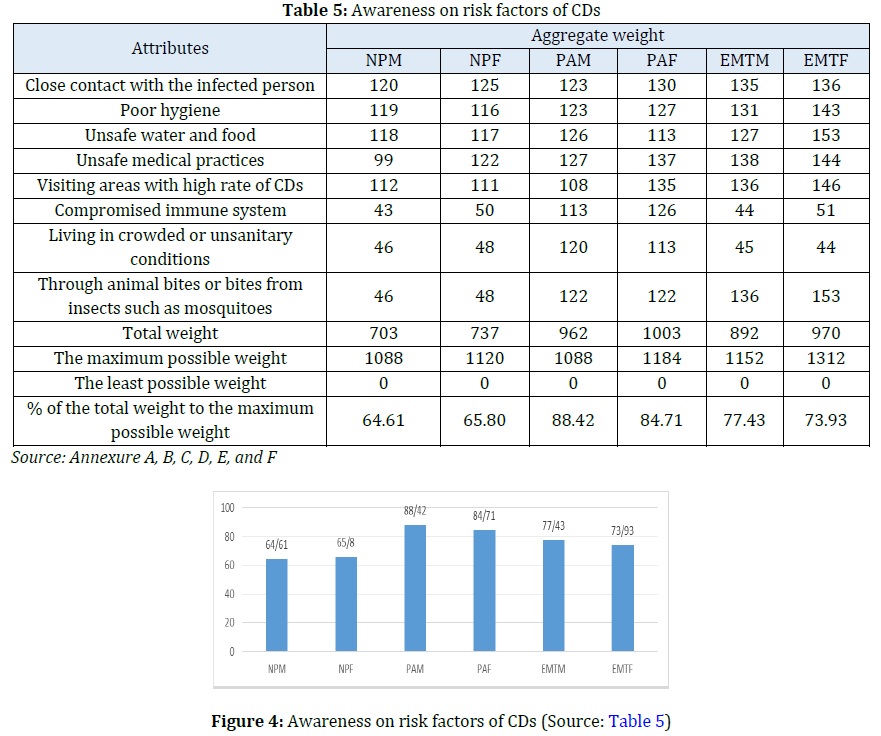
This shows in the case of NPM and NPF poor awareness level related to the risks such as compromised immune system, living crowded and unsanitary conditions, and through animal bites, etc. Similarly, in the case of EMTM and EMTF, there is a less awareness of compromised immune system, living crowded and unsanitary conditions.
Suggestions for improving the awareness level of paramedics
Based on the findings of the study it seems to be the paramedics are lacking the awareness of symptoms of communicable diseases as compared to the types of communicable diseases and risk factors. In this regard, the following initiatives may be undertaken to overcome the issue.
- Regular counselling by the team of expert doctors.
- Proper communication through advertisement in various important places of the hospital in vernacular language and English language.
- Regular cleaning of hospital premises.
- Proper sanitation in the hospital premises.
- Immediate support in case of any staff suffers any of communicable diseases.
- Besides, the other innovative initiatives which will help to reduce and control the communicable diseases among the paramedics.
Scope for future study
The study can be undertaken in the government run hospitals. The study can be only undertaken for the doctors. Similarly, the study can be further undertaken in other sectors.
Limitations of the study
The present study is limited to the selected hospitals in the study areas of eastern part of India. The sample size is also limited to 217 and if the composition of sample size increases and the demographic profile change, the result may be different.
Conclusion
In academic research search for excellence, the present study helps to develop new ideas and innovative findings. Accordingly, in the case of CDs the awareness of symptoms, the majority is aware of symptoms like fever, cough, difficulty in breathing, and vomiting. However, very less awareness was found on fatigue, body aches, nausea, diarrhea, rash, and painful stores in skins and for awareness level of types of CDs, highly awarenee of COVID, bacterial infections, fungal infections, and viral infections was evident. However, there is less awareness level for the parasitic infections and prion infections as well as in the case of NPM and NPF poor awareness level related to the risks such as compromised immune system, living crowded and unsanitary conditions, and through animal bites, etc. Similarly, in the case of EMTM and EMTF, there is a less awareness of compromised immune system, living crowded and unsanitary conditions. This requires more counselling for these CDs.
Disclosure Statement
No potential conflict of interest was reported by the authors.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' Contributions
All authors contributed to data analysis, drafting, and revising of the paper and agreed to be responsible for all the aspects of this work.
Orcid
Soumya Ranjan Ray Choudhury
https://orcid.org/0000-0002-8454-3955
Chandra Mohan Patnaik
https://orcid.org/0000-0002-5979-0989
Ipseeta Satpathy
https://orcid.org/0000-0002-0155-5548
HOW TO CITE THIS ARTICLE
Soumya Ranjan Ray Choudhury, B. Chandra Mohan Patnaik, Ipseeta Satpathy. Communicable Diseases (CDs) Among Paramedics in Private Healthcare in India. J. Med. Chem. Sci., 2023, 6(9) 1967-1974
)