Document Type : Original Article
Authors
1 Research Scholar, KSoM, KIIT Deemed to be University, Bhubaneswar, Odisha, India
2 KSoM, KIIT Deemed to be University, Bhubaneswar, Odisha, India
3 Senior Professor, KSoM, KIIT Deemed to be University, Bhubaneswar, Odisha, India
Abstract
Quality of life is a relative term. The relevance of it changes as per the situation. The present paper tried to capture different aspects of QoL in the case of breast cancer patients of rurban (rural and urban) investor communities in the study area. The study was undertaken to understand the impact quality of life of breast cancer survivors in rurban areas of Odisha, India, to understand whether any difference of opinion exists among different age groups in the rurban areas considered for the study and contributing to the prevailing literature. The entire data were captured under three constructs such as physical health, mental health, and the impact of spirituality on breast cancer patients for improving the survivors’ quality of life. The results found that most respondents opined that fatigue, sleeping problem, anxiety, body pain, fear of uncertainty, and weakness were the most common issues faced by the BC survivors. It was also observed that the medical support is more for urban BC patients than rural ones. At the same time, there is a more positive mindset for the rural patients compared to the urban respondents in the study areas.
Graphical Abstract
 of Breast Cancer (BC)survivo ... ', 'data/jmcs/coversheet/391666252557.jpg'))
Keywords
Introduction
There are 5,22,000 cases of breast cancer each year worldwide, making it the fifth leading cause of death among females [1]. There are 1,98,000 deaths per year due to this disease in developed countries after lung cancer [2]. 20 to 24.5% of cancer deaths among women in developing countries are caused by breast cancer [3]. Although breast cancer mortality rates are proportional to factors including age, diagnosis stage, treatment efficiency, etc., they are highly variable [4]. Developmentally disadvantaged women have different tumor behaviors, treatment responses, prognoses, and clinical manifestations. The lack of knowledge about breast cancer's etiology is the reason for this [5]. The age at which breast cancer is first detected in developed countries is generally 60. Cancers of the lung and colon are typically diagnosed at 70 and 68, respectively, much earlier than lung and colorectal cancer. Breast cancer is diagnosed in 19% of women between the ages of 30 and 49. Additionally, they are detected in all women over 65 years of age. Surgery or mastectomy is the primary treatment for women under 40 with breast cancer. many older women also do not prefer radiation therapy due to fears of recurrence or fear of radiation [6, 7].
Stages I, II, and III of breast cancer are the most common diagnoses for breast surgery, while stage IV patients must undergo hormone therapy. Improved diagnosis and treatment procedures have increased breast cancer survival rates in the USA from 78% to 89%. Several physiological changes have been observed in breast cancer survivors, including reduced feeling, tightness in the arms, shoulders, and chest wall, fatigue, and cognitive impairment [8-10]. Infertility, osteoporosis, and even neuropathy may result from chemotherapy treatment [11, 12]. Atrophic virginities and dyspareunia can be reduced with hormonal treatment [13, 14].
Researchers have linked physical activity to improved health in breast cancer survivors. Physically active survivors have been shown to live longer and healthier lives than those who were not. Exercise has been shown to increase the chances of a breast cancer patient maintaining a healthy life over a long period [15]. Furthermore, studies have demonstrated that lifestyle preferences associated with cancer are negatively correlated with anxiety and overall well-being. As they associate breast cancer with lifestyle troubles, women realize that lifestyle choices could have contributed to its spread [16-18]. Spirituality allows us to interact with the world and unite with it. Human life is made meaningful and valuable by interaction and assimilation. Individuals are given policies and spiritual practices through moral/spiritual gathering therapy, which help them attain a nonmaterial understanding of themselves, the world, events, and appearances, thus enhancing their sense of fulfillment and well-being [19]. To deal with cancer’s physical and psychological consequences, patients should rely on spirituality [20]. Psychological adjustment and endurance may be negatively affected by insufficient social channels and understandings [21-24]. There is a correlation between the death rate of breast cancer and social connections, social maintenance, and general well-being [25-27]. Few studies in Indian literature examine the factors that cause breast cancer, particularly in the study area. In the Indian context, factors of life quality studied previously regarding BC survivors do not apply due to living styles, family status, social and cultural values, healthcare facilities, etc [28].
Review of earlier studies
As a result of BC diagnosis, patients and their families suffer significant physical, mental, and economic consequences. People's lifestyles and even their families’ dynamics must change due to these consequences [29].
Besides physical and psychological well-being, QoL also includes social well-being. A person's quality of life has been defined in many ways; however, according to the WHO, it is their perception and satisfaction with life and their general assessment of how well they are functioning [30].
Despite an increase in cases each year, breast cancer (BC) remains one of the most prevalent malignant tumors among women worldwide, with the highest mortality rate. According to the latest data on cancer worldwide for 2020, there will be 2.26 million newly diagnosed cases of BC, surpassing lung cancer (11.7%) [31].
As a result of their treatment experiences and associated symptoms, BC patients' mental health is also negatively impacted. Even years after an acute phase or successful treatment, BC patients report high anxiety, depression, and distress levels [32].
In addition to their survival, women's quality of life can affect the cohesion of their families as they are the most significant members of the family. Consequently, psychosocial problems are associated with twofold increased severity of physical symptoms. Upon diagnosis, patients often experience devastating and intolerable treatment symptoms [33].
Family caregivers of cancer patients may experience physical, mental, and spiritual difficulties, which, if neglected, may have serious consequences for the entire family. Caregivers' physical and mental health will substantially decline if they are left without appropriate treatment and intervention-they will become "hidden patients." According to the findings, family caregivers were less likely to suffer depression, anxiety, and stress after the cognitive behavioral intervention [34].
In addition to being implicated in the cell cycle, apoptosis, and proliferation, the growth arrest-specific 2 (GAS2) gene may also promote cancer progression. Nevertheless, it is unknown whether GAS2 contributes to the progression or prognosis of colorectal cancer. As a result, this study examined the association between GAS2 expression in tumors and the progression and prognosis of CRC [35].
A transition occurs when a state, condition, or place changes. It is common for chronic disease patients to experience transitions, for example, patients with end-stage renal disease. Through effective factors such as the development of management strategies, hemodialysis patients will receive more specialized care. Nursing interventions will be more appropriate, and training programs will be more effective in preparing patients and their families for the transition to hemodialysis [36].
Research objectives
To study the impact quality of life of breast cancer survivors in rurban (rural and urban) areas of Odisha, India.
To understand whether any difference of opinion exists among different age groups in the urban (rural and urban) areas considered for the study.
To contribute to the existing literature
Scope of the study
This study was conducted in Odisha, India. The study was restricted to rurban (rural and urban) areas of Cuttack district and Khordha district. A total of 8 blocks constitute the Cuttack district, including Baranga, Cuttack Sadar, Kantapada, Mahanga, Niali, Nischintakoili, Salepur, and Tangi-Choudwar. Similarly, in the Khordha district, Tangi, Khordasadara, Banapur, Begunia, Bolgarh, and Chilika were considered in addition to respondents from Cuttack and Bhubaneswar cities included. Only those participants of the investor community in the study areas who had breast cancer were included. Those who were open to the survey considered it includes all the female age groups from 20-60 years of age.

With reference to Table 1 Under breast feeding 77.98% participants were breast feeding and rest were not feeding. For the family history 31.19% having don’t have family history and rest were having family history. In case of age group majority participants from 31-50, followed by 20-30 and rest were above 50. Similarly, 3 or more abortion 37.15%, 29.81% having 2 times, 19.67% for one time and rest were no abortions. In case of 76 respondents having 3 or more children, 51 respondents having 2 children, 66 respondents having single child and 25 respondents having no child. In case of 61 respondents having more than 5 pregnancies, 54 were 3-4 pregnancy, 73 having 1-2 pregnancy and 30 were no pregnancy. Majority of participants were upper class, followed by middle class and rest were lower class. Similarly, majority were married, followed by unmarried and divorce.
Methodology of the study
The current research is based on secondary as well as primary data. The data were collected by visiting various libraries and online mode by visiting various websites. For collecting primary data initially, 29 variables were identified from the review of the literature and 5 core group discussions consisting of 6 members each. The same questionnaire was used for conducting the pilot study among the rurban population by taking 53 respondents from the initial variables; however, after the pilot study, 22 variables were retained. Five-point Likert-type scale method was used for the computation of data along with an Anova test, and this purpose score of 5 for completely agree (CA), score 4 for agreeing (A), score 3 for neutral (N), score 2 for disagreeing (DA) and score 1 for completely disagree (CDA). Forthe collection of desired data, 412 questionnaires were distributed; of that 239 responses were received which was 58%. However, 218 responses were received in proper form. The total period of study was 4 months, i.e., May 2022 to August 2022. The sample for the current research was collected through non-probabilities sampling, precisely through the convenient sampling technique. With reference to Table 2, first 4 weeks concentrated for the conceptualisation and outline of research work. Next one month was for extensive literature review, following next one month was focused on gap analysis and data collection phase and last one month was data analysis and conclusion of the paper work done.

The sample size for the unknown population
This study will calculate the sample size as a ratio between 1:4 and 1:10 (Rummel, 1970; Schwab, 1980). In the above method, the minimum sample size is four times the items, and the maximum sample size is ten times the items. In the present case, 22 core variables are included; accordingly, the sample size should be 88 to 220. This indicates that the present 218 responses were within the desired sample size.
Hypotheses
Based on Physical well being
H0: There is a significant difference of opinion between Breast Cancer survivors based on the positive impact of quality of life and physical well-being.
H1: There is no significant difference between Breast Cancer survivors based onthe positive impact of quality of life and physical well-being.
Based on mental health assessment
H0: There is a significant difference of opinion between Breast Cancer survivors based onthe positive impact of mental health assessment.
H1: There is no significant difference of opinion between the Breast Cancer survivors based on the positive impact of mental health assessment.
Based on spiritualism
H0: There is a significant difference of opinion between Breast Cancer survivors based onthe positive impact of spirituality.
H1: There is no significant difference of opinion between Breast Cancer survivors based on the positive impact of spirituality.
Based on physical well being
H0: There is a significant difference of opinion exists between Breast Cancer survivors based on the positive impact of quality of life and physical well-being.

Figure 1: Breast cancer stages and symptoms



Figure 2: Percentage of total weight to maximum possible weight for different parameters (Source: Table 4)
H1: There is no significant difference exists between Breast Cancer survivors based on the positive impact of quality of life and physical well-being.
The p-value in Table 5 is less than 0.05, as well as the F-calculated value of 44.73312, which is higher than the F-critical value of 3.4668. It follows that the hypothesis that breast cancer survivors have significantly divergent opinions on the quality of life and physical well-being is rejected. As a result, both qualities of life and physical well-being are positively impacted regardless of age.
Based on mental health assessment
H0: There is a significant difference of opinion exists between Breast Cancer survivors based on the positive impact of mental health assessment.
H1: There is no significant difference of opinion exists between the Breast Cancer survivors based on the positive impact of mental health assessment.


The p-value in Table 6 is less than the threshold of 0.05, and the F-calculated value is 812.35, which is higher than the F-critical value of 2.53. In light of the positive impact mental health assessments have on cancer survivors, a significant difference in opinion does not exist. So, mental health assessment, irrespective of age, has a positive impact.
Based on spirituality
H0: There is a significant difference of opinion between Breast Cancer survivors based on the positive impact of spirituality.
H1: There is no significant difference of opinion between Breast Cancer survivors based on the positive impact of spirituality.
Table 7 shows that the p-value is less than 0.05 level, as well as the F-calculated value of 797.61, which is higher than the F-critical value of 2.53. Therefore, the hypothesis that a significant difference of opinion exists considering the positive impact of spirituality on breast cancer survivors is rejected. So, spirituality, irrespective of different ages, has a positive impact.
Figure 1 presents the various stages and symptoms. This includes fatty tissue, lobe, nipple, muscle and leads to breast cancer.
Results and Discussion
With reference to Table 4, On the questions about the quality of life and physical well-being of survivors of breast cancer, actual weighted scores to maximum possible scores for urban females aged 20-30, urban females aged 31-50 and over 50 years were respectively 79.11%, 83.94%, and 89.72%, and for rural respondents of similar ages were 92.25%, 87.38%, and 93.27%. It suggests that the various variables considered for the study positively affected the BC survivors irrespective of the age group of urban and rural people.






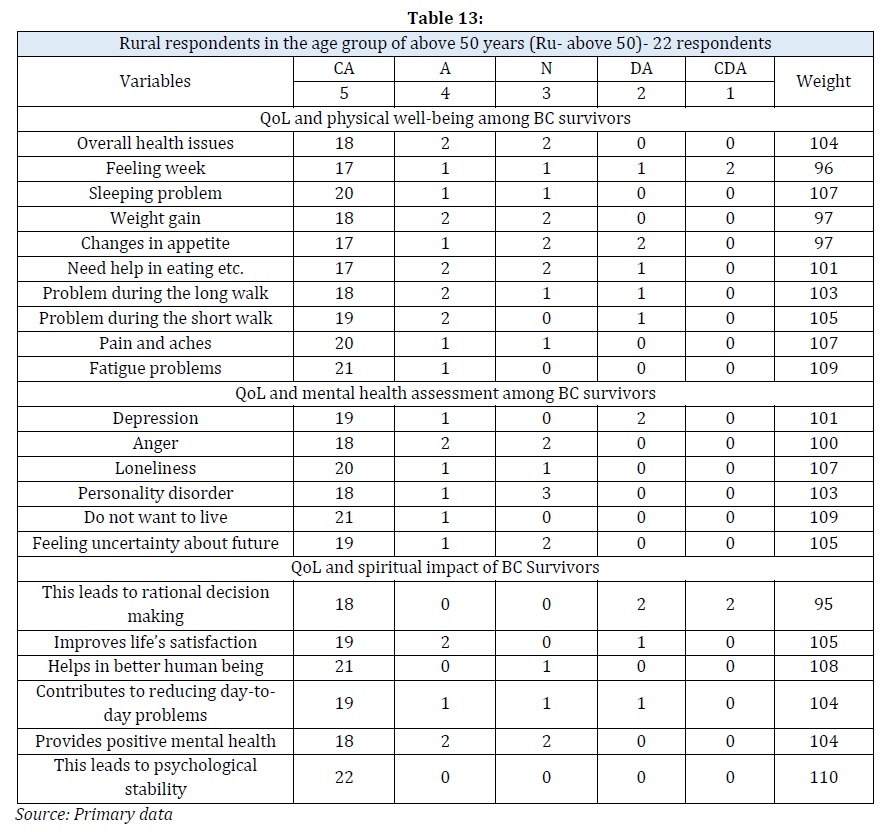
As regards the QoL and mental assessment among BC survivors, it is noted that the actual weighted score to the maximum possible score for the rural female age groups of 20-30 years, 31-50 years, and over 50 years was 94.03%, 94.44%, and 94.70% whereas the same for the urban female age groups was 81.11%, 92.45%, and 93.45% respectively. This concludes that both rural and urban women believe that all the attributes included under this parameter are relevant for the BC survivors.
Joining the query related to the quality of life and spiritual impact on BC survivors, it was found that the actual weighted score to the maximum possible score for the urban age group of 50 and above, between 31-50 and 20-30, was 91.61%, 90.39%, and 980.09%. The rural participants’ figures were 94.85%, 91.97%, and 93.89%, respectively. The quality of life of survivors does appear to be greatly impacted by spirituality.
Conclusion
Quality of leading life is a challenge for the patients and their near and dear ones for breast cancer survivors. The present study addresses the various aspects of health, mental health, and spirituality. These aspects have an impact on improving the quality of life of breast cancer survivors under three parameters. During the study, it was found that urban patients are better placed than rural patients. This is mainly the availability of super specialist hospitals in the urban areas and the same being deprived in the rural areas. In some cases, it was also found that breast cancers survive over 90 years of age in rural areas. This may be due to lifestyles in rural areas and food habits. However, the ground reality is that we need to extend all the possible support to these people so that there will be scope for living longer life as they also deserve to live in society. Family members also suffer a lot if any causality happens to any one of the dear members of the family. The family members of the patients have to lead their whole life without the person they love very much. So, all these can be resolved with social support, creating awareness, and providing affection. We cannot change the destiny but can try to give our best to the patient during her life period.
Acknowledgments
We are thankful to all the participants of the rurban areas of Cuttack and Khordha districts of Odisha, India. Without their active participation, it could not have been possible to complete the present paper.
Funding
This research did not receive any specific grant from public, commercial, or not-for-profit funding agencies.
Authors' contributions
All authors contributed to data analysis, drafting, and revising of the paper and agreed to be responsible for all aspects of this work.
Conflict of Interest
There are no conflicts of interest in this study.
ORCID
Aditya Prasad Sahoo
https://orcid.org/0000-0003-4399-2604
B.Chandra Mohan Patnaik
https://orcid.org/0000-0002-5979-0989
Ipseeta Satpathy
https://orcid.org/0000-0002-0155-5548
HOW TO CITE THIS ARTICLE
Aditya Prasad Sahoo, B. Chandra Mohan Patnaik, Ipseeta Satpathy. Quality of Life (QoL) of Breast Cancer (BC) Survivors of the Rurban in Vestor Community in India. J. Med. Chem. Sci., 2023, 6(5) 946-961
https://doi.org/10.26655/JMCHEMSCI.2023.5.2
URL: http://www.jmchemsci.com/article_159213.html
)